Part 3: Delta Variant Hot Surge Summer in the U.S.
The Delta Variant Takes Over as COVID Cases and Hospitalizations Surge Across the Country

This is the third part to the articles Delta Variant Dominance in the U.S. and Part 2: Delta Variant Dominance in the U.S. and Unvaccinated Vulnerability.
Big Picture
One month after Delta becoming the dominant strain in the United States, the summer surge is underway. We are experiencing exponential growth and at this rate are estimated to reach our Winter peak in a month’s time under current conditions. The regional hotspots are growing larger and every state in the country is increasing in cases. The data from hotspots are consistently showing the overwhelming amount of cases and hospitalizations are amongst those unvaccinated with demographics trending younger. Delta has increased the rate of admissions to ICUs causing them to reach capacity sooner in multiple states and patients are being sent to other hospitals for care, and data suggests that counties with higher vaccination rates may also reach capacity sooner than in previous waves putting the larger healthcare system across the country at risk. Transmission, severity, and immune escape continue to be a challenge for controlling spread with only vaccines and some counties have begun implementing the World Health Organization’s recommendation of indoor masking. Vaccinations rates have slowed to levels not seen since December while most counties maintain low vaccination percentages across their populations. Under the current conditions, the transmissibility of Delta, and the effectiveness of vaccines against infection, herd immunity is estimated to be highly unlikely suggesting an increased likelihood of exposure and the urgency of vaccinations to develop immune protection against symptomatic disease, hospitalization, and death. A significant portion of the population including children that get COVID continue to experience the persisting symptoms of long covid and recent research supports previous data it can result in damaged gray matter in the brain. With the growth of Delta as the dominant strain across the world, the issue of vaccine equity becomes a greater humanitarian crisis with billions of people without immune protection from the vaccines and high levels of transmission creating the potential for variants that can scale back the progress we have made with vaccinations. We are at an inflection point of this surge in the United States and around the world and urgent action is needed to suppress transmission to save lives, prevent long-term disease from COVID, and improve the social and economic impacts on our greater society.
Caveats: Prevalence numbers are only estimates due to a very small percentage of COVID tests being sequenced across the country and lag in reporting data. Additionally, studies on vaccine effectiveness and severity cited in this article continue to be early and in large part preliminary and studies are ongoing to provide greater details on transmissibility, immune escape, and severity. Vaccine breakthrough infections reported to CDC are likely underreported since national surveillance relies on passive and voluntary reporting and is only recommended for those who are symptomatic and not those who are exposed. Projections on herd immunity and hospitalizations are limited due to incomplete data and a changing landscape with dynamic variables. Long covid studies for adults and children continue to be underresearched and more data is need to provide greater understanding in this area. Any updates to the key points from past Delta publications are addressed in the body of this piece.
Overview of Key Points from Past Delta Publications
Key points from Part 1: Delta Variant Dominance in the U.S.
- Genomic sequencing data and weekly growth rates were used to estimate when the Delta variant would become the dominant strain
- Being fully vaccinated provides high levels of immune protection although lower than previous strains (e.g., Pfizer: 93% against Alpha, 88% against Delta) and much lower if partially vaccinated (e.g., Pfizer and AstraZeneca only 33% against Delta)
- U.K. data shows most COVID cases largely amongst those unvaccinated
- Early and preliminary data shows Delta, in comparison to the original wild-type that started the pandemic, has increased levels of transmissibility by nearly 4 times, increased severity around 3.3 times, and increased immune escape that reduces previous immune protection
- The United States remains largely vulnerable to Delta due to low vaccination rates in many counties and states that are affected by access, trust, and misinformation
- Recommendations include increasing genomic testing, testing the fully vaccinated to increase data on variants of concern that could evade immunity and increase data on secondary infections, increase ventilation in buildings, and recommending of quality masks (e.g., N95s)
Key points from Part 2: Delta Variant Dominance in the U.S. and Unvaccinated Vulnerability
- UK and US both bottomed out on decreasing cases at the point that Delta became dominant
- Daily count of vaccinations dropped to January levels
- Unvaccinated vulnerability highlighted by the 90% of U.S counties having less than 50% of their populations fully vaccinated and vaccination rates ranging between 9%-70%
- Cases increasing in Missouri, Kansas, Oklahoma, and Arkansas with some of their counties seeing surging case increases
- Breakthrough cases can happen due to vaccines not being 100% effective and factors like an individual’s immune response to the vaccines, viral load exposure by amount and time, and the virus’s enhanced ability to bind to the ACE2 receptor
- Masking recommendation by World Health Organization rationale supported by Delta’s increased transmissibility and immune escape which increases the number of breakthrough cases and potential for infectiousness
- Cases are trending younger largely due to younger demographics having a lower percentage of their populations vaccinated compared to older populations
- Long covid can affect roughly 23% of the population with persisting symptoms ranging from fatigue, shortness of breath, “brain fog”, sleep disorders, fevers, gastrointestinal symptoms, anxiety, and depression
- Vaccines work as supported by data showing the overwhelming amount of cases and hospitalizations amongst the unvaccinated and superspreader events where the vaccinated did not become infected
- Recommendations include increasing genomic testing, implementing quality mask recommendations for indoor use, increasing ventilation, and testing the fully vaccinated after exposure to improve data on vaccine effectiveness against new variants and increase data on secondary infections
Delta Prevalence Levels
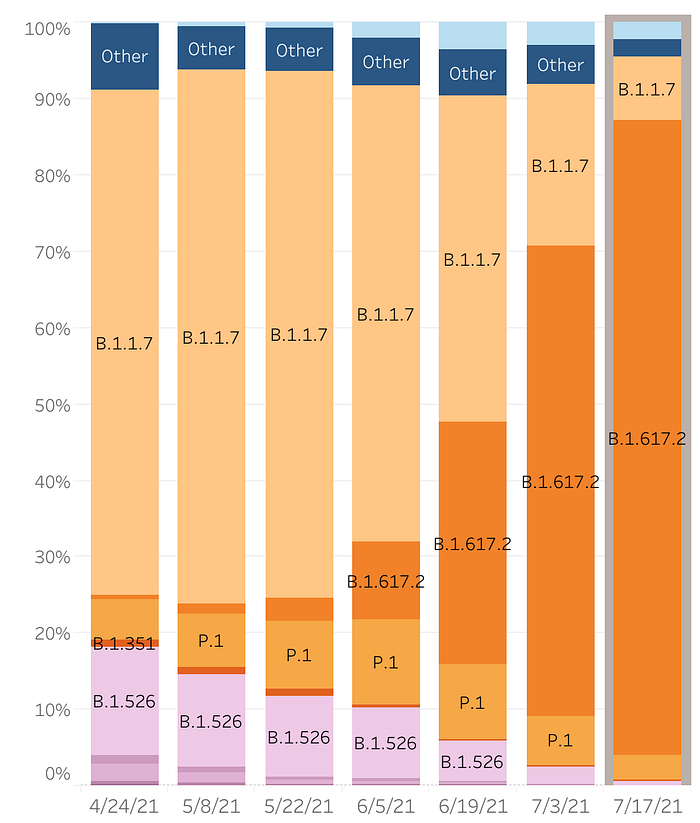
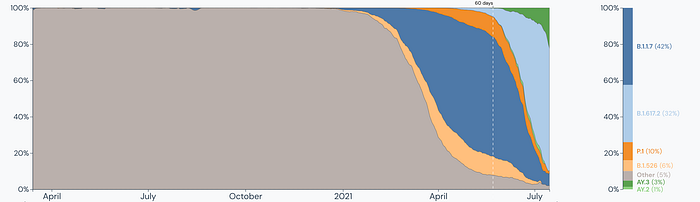
The latest genomic sequencing data available from Outbreak.info puts Delta (B.1.617.2) at around 69% prevalence as of July 14th. If we include its sublineages, which we introduce at the end of this publication, Delta makes up closer to 91% of all the current cases in the United States.

On July 21st, the CDC estimated Delta was at 83% prevalence as of July 17th in the United States.
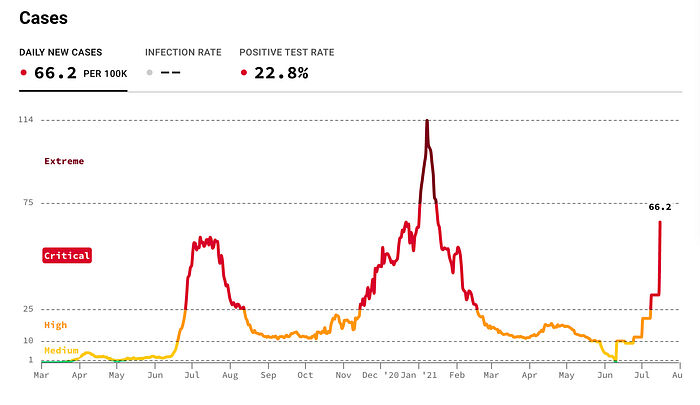
Cases Surge
On July 21st, we reached nearly 40,000 daily new cases on a 7-day rolling average, an increase of about 60% over one week and an increase of 160% over the last weeks. We are outpacing the 7-day rolling average for UK’s new daily cases and are expected to soon surpass them.

However, when we look at daily new cases without the 7-day rolling average we see that on July 16th, we reached nearly 80,000 new daily cases just on that day, double that of the July 21st 7-day rolling average.
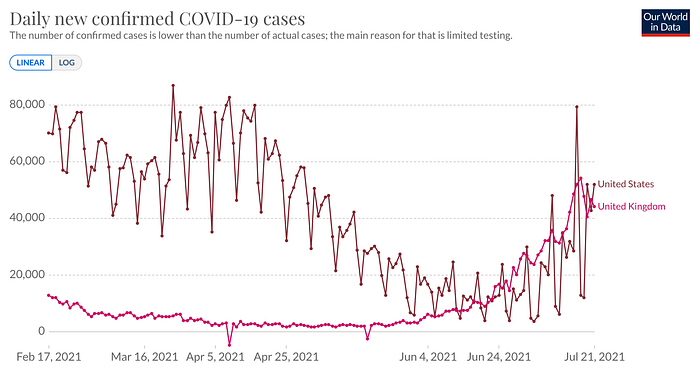
If we calculate our growth from when we bottomed on decreasing cases on June 22nd through the 7-day rolling average with 11,299 new daily cases, we’ve grown by nearly 4 times over the course of a month. A weekly growth rate of 60% comes out to an increase of about 410% over a month. If this stays consistent, we can estimate that in a month from now the nearly 40,000 daily new cases will become roughly 164,000 daily new cases on a 7-day rolling average. If we see peaks double the 7-day rolling average as we recently have, it is possible to see us reach a peak of around 328,000 daily new cases within a month.
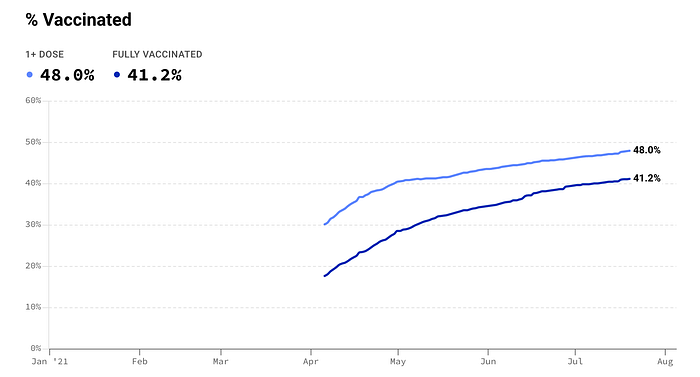
Vaccination Rates
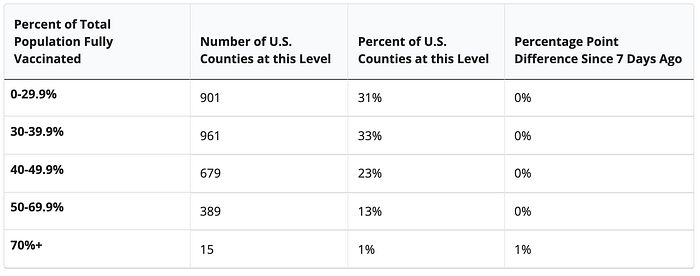
Vaccinations continue to stall with 87% of counties having less than 50% of their residents fully vaccinated and only 1% of counties having more than 70% of their residents fully vaccinated.
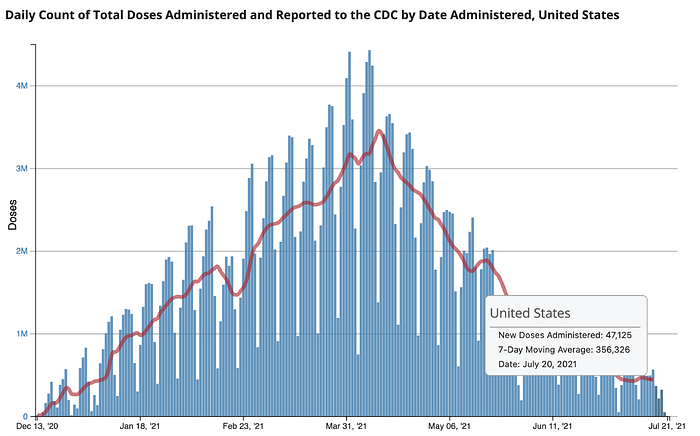
The percent of those fully vaccinated is changing at an increasingly slow pace as we see the daily count of total doses administered drop to levels not seen since the first three weeks of the release of the vaccines, a time when there were only two groups eligible, healthcare workers and long-term care residents. As of July 20th, the 7-day moving average sits at 356,326.
At this time, less than half of the population is fully vaccinated, roughly 48% and 7.4% are partially vaccinated against COVID-19, a total of 55.4% who have received at least one dose.


The challenge here becomes clear when we compare the vaccination rates to the roughly 333 million population in the United States. With 161 million people currently fully vaccinated, this means that 172 million remain vulnerable without full protection from the vaccines and with 186 million people receiving at least 1 dose, that means 147 million people have no immune protection from the vaccines. To put this number of people into perspective, the UK is roughly 68 million people, so if you can imagine the UK being two and a half times its total population size which would be 173 million people and picture all those people not being fully vaccinated, that is the current challenge and vulnerability we are presented with here in the United States.


Regional Hotspots
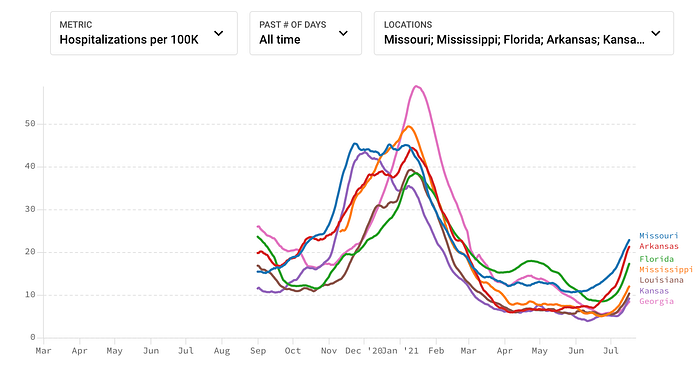
The Regional hot spots are expanding beyond the lower midwest and southern states of Missouri, Kansas, Arkansas, and Louisiana to include the southeastern region of the United States with the addition of Florida, Tennesse, Georgia, and Alabama, and a new regional hot spot is emerging with Nevada and California.

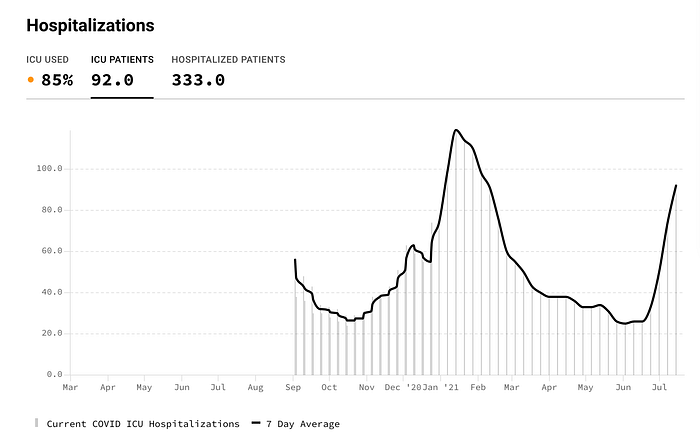
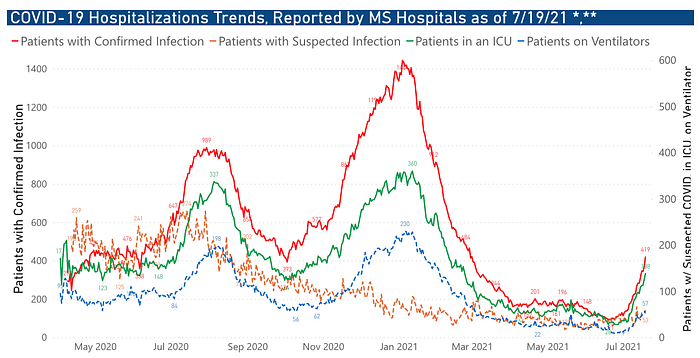
Hospitalizations also continue to climb for many of the states in the regional hotspots with the chart below indicating a faster climb than during the winter surge. Missouri, Arkansas, and Florida have the highest levels of hospitalizations and are quickly approaching half the numbers as the previous surge.
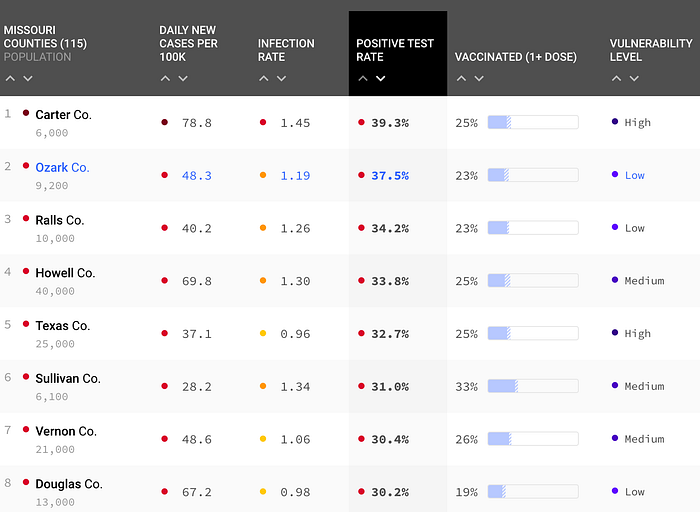
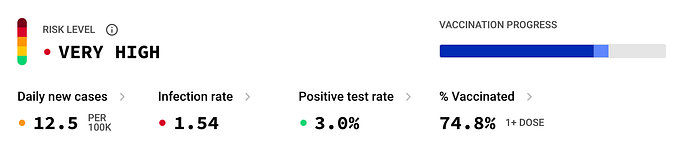
Missouri continues to be surging with several counties above 30.3% of their tests coming back positive, as high as 39.3% in the county of Carter. In one county you have as high as 96 daily new cases per 100k people and in another county the infection rate is as high as 1.47.
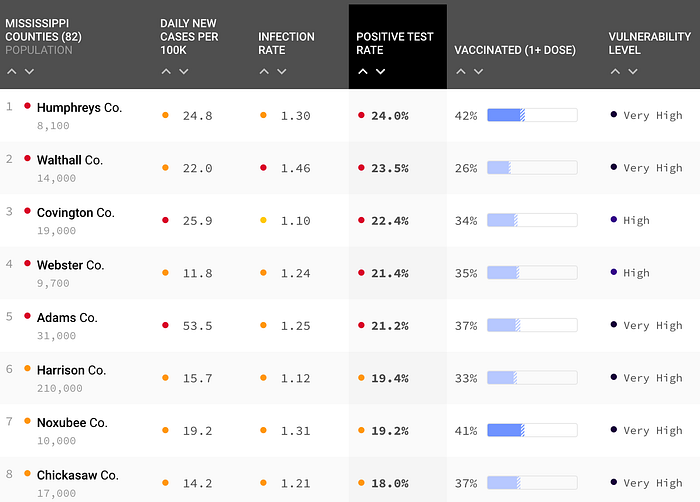
In Mississippi, we see a similar story with some counties having almost a quarter of their COVID tests coming back positive while the infection rate is as high as 1.50 in other counties and another county reaching up to 53.5 daily new cases per 100k people.
Florida Surges and ICUs run out of capacity
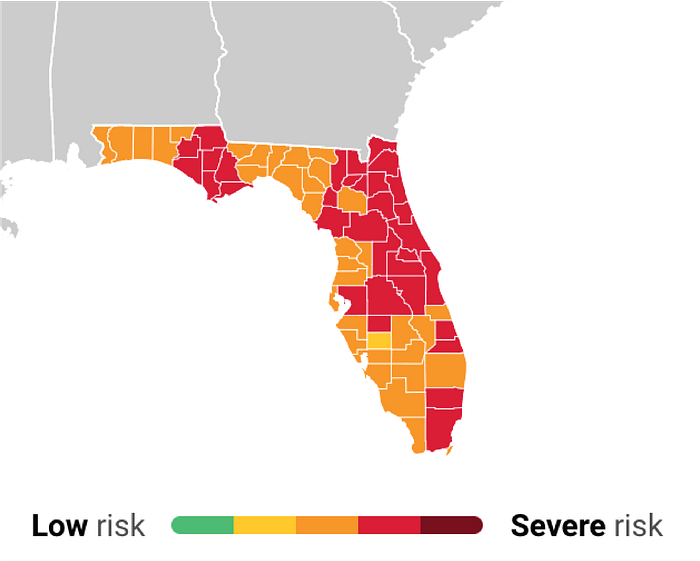
The County of Duval is one of many experiencing high levels of cases and hospitalizations.
Community leaders are emphasizing the high levels of hospitalizations and are pleading with their residents to use the vaccine as a better solution.
“We are seeing hospitalizations for this virus here in Jacksonville at a level we have not seen since the height of the pandemic last year. We have a better solution that is going around, a solution that prevents severe illness and death, and that is the vaccine.” -Mayor Lenny Curry of Jacksonville, Duval County.
Current vaccination rates are around 41% fully vaccinated and 48% with at least one dose. Duval County has close to 1 million residents, which means that roughly 600,000 remain not fully vaccinated.
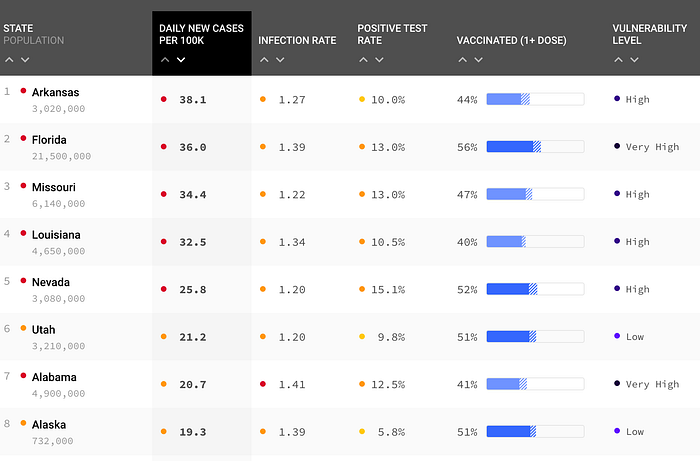
Florida is currently ranked second-highest state for daily new cases per 100k with 6 of the top 10 being in the regional outbreak of the lower midwest, south, and southeast states including Arkansas, Missouri, Louisiana, Alabama, and Oklahoma. The other four states include Nevada, Utah, Alaska, and Arizona.
Vaccinations for the state of Florida currently sit at 47.9% fully vaccinated and 55.7% with at least one dose. If we put this into proportion of the overall state population of about 21.5 million, this leaves a little more than 11 million people not fully vaccinated and about 9.5 million with no immune protection from a COVID vaccine.
Every State Increasing
It is now evident that every state, including those with higher vaccination rates, is increasing its case numbers. Different states have varying vaccination rates, different prevalence levels of Delta, and recently some states have counties with additional nonpharmaceutical interventions like indoor mask-wearing. All of these factors play a role in the rate at which Delta spreads as well as the extent to which areas become a hotspot and hospitals reach capacity. What is clear is that there is no state that has reached levels of vaccination rates that prevent an increase in cases, transmission, and hospitalizations. Many health experts are calling for nonpharmaceutical interventions like masking indoors and improved ventilation and air filtration in addition to vaccinations in order to suppress surging cases.
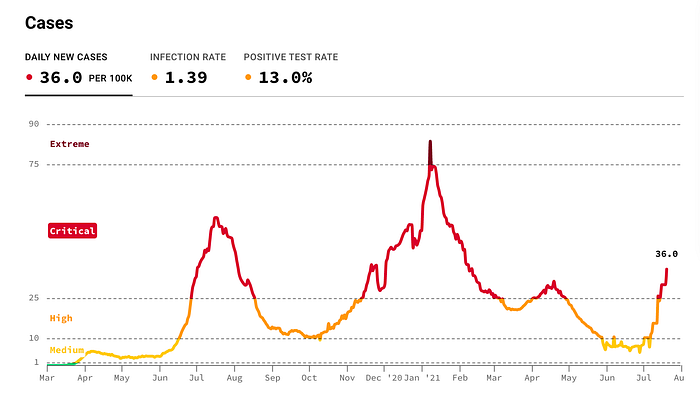
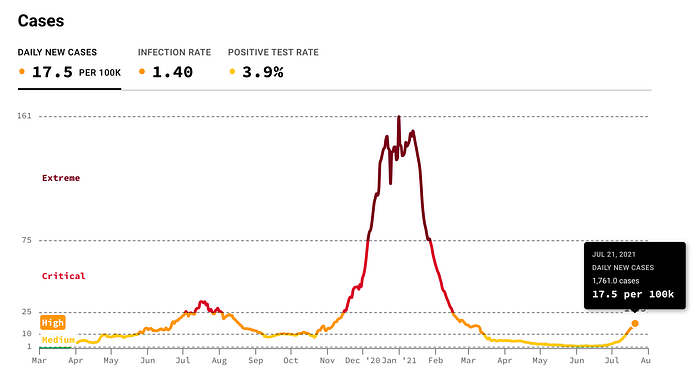
Even counties like Los Angeles that have a higher vaccination rate than the United States does nationally announced in a press release on July 21st that new daily cases have surged 20-fold in a month from 124 new covid cases on June 21 to 2,551 new covid cases.
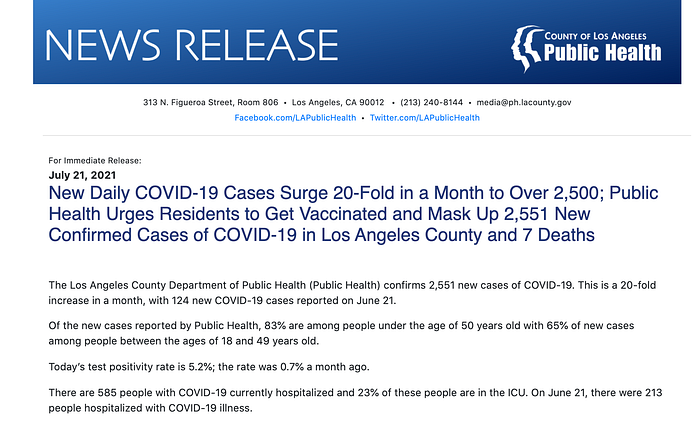
On July 21st, Los Angeles County had the most COVID cases it’s had in the last six months.
Delta Transmission and Severity Update
A recent study showed that the viral load of Delta is upwards of 1,000 times higher than that of the original wild-type that started the pandemic.
“The investigation on daily sequential PCR testing of the quarantined subjects indicated the viral load of the first positive test of Delta infections was ∼1000 times higher than that of the 19A/19B strains infections back in the initial epidemic wave of 2020, suggesting the potential faster viral replication rate and more infectiousness of the Delta variant at the early stage of the infection.”
This study may support instances of ‘fleeting exposure’ of the Delta variant which suggests brief exposure time needed to become infected as documented recently in Australia by Dr. Kerry Chant, New South Wales Health Officer, at a recent press conference.
“…the initial case was highly infectious as transmission must have occurred from ‘fleeting exposure,’ noting that the woman who caught the infection at the cafe was seated outside and there was no known exposure with the initial case.”
A Singapore study that is being submitted for international publication showed the following results for Pfizer and Moderna:
- 69 percent effective against infection regardless of symptoms
- 80 and 90 percent effective against symptomatic disease
- 93 percent effective against severe COVID-19 disease which includes requiring oxygen supplementation, ICU care, or death.
These numbers align closely with the effectiveness data for symptomatic disease and hospitalization that has been released for the UK and Scotland by Public Health England although their data was a mix of AstraZeneca and Pfizer which showed 80% effectiveness against symptomatic disease and 94% effectiveness against hospitalization for those who are fully vaccinated.
While data from the Public Health UK shows an increase in hospitalizations for those infected with Delta, we are still waiting on more data to see if it leads to more deaths. A recent study provides data based on animal models that it is more severe and that the virus has increased ability to bind to the ACE2 receptor cells making the virus easier to infect its host. Although this study is limited because it was conducted with hamsters and not humans, it gives us some insight into the potential mechanisms by which Delta may be interacting with humans.
Herd Immunity
The hope of herd immunity grows dimmer with increased transmissibility of the Delta variant and increased immune escape against the vaccines. The original percentage of 70% fully vaccinated needed to achieve immune protection was based on the wild-type that started this pandemic having an R0 or reproduction number of 3. This means that for one person infected, that person is expected to infect 3 more people. Additionally, the efficacy of vaccines in preventing infection was 95% for the most effective vaccines we had like Pfizer’s mRNA vaccine. These numbers have changed due to Delta’s reproduction number estimated between 6–8 and vaccine effectiveness against symptomatic disease decreasing to levels between 80–88%, we can recalculate the percentage needed of fully vaccinated individuals in order to reach herd immunity. Using the herd immunity formula of (1/E) x (1–1/R) where E is vaccine effectiveness in reducing transmission and R is the reproduction number or R0, we get (1–1/3)/.95=70% with the original wild-type. Adjusting the numbers for Delta, we can see that the calculation for reaching herd immunity shows that under these conditions it is unlikely (1–1/6)/.88=94% if not impossible to reach herd immunity, (1–1/8)/.80=109%. With the 94% fully vaccinated number to reach herd immunity, I applied an estimate of the best-case scenario for the reproduction number (R0) and effectiveness against transmission while in the second calculation I applied an estimate of the worst-case scenario which shows it is not possible to reach herd immunity.
During a recent interview, Dr. Michael Osterholm, Director of CIDRAP shared his thoughts on reaching herd immunity,
“I, for one, don’t believe we’ll ever reach herd immunity… herd immunity means having enough people protected… where you don’t see ongoing increases of transmission… and I think for this virus as we see how infectious it can be with the variants… what will do is dramatically decrease transmission [with vaccinations], we will make it very different than it has been.”
Assuming we did reach herd immunity in our country, our “herd” mixes with other herds. In other words, being in a global community with international travel, our herd interacts with other herds or, in other words, countries across the world which pose another challenge for achieving herd immunity and highlights the importance of achieving high vaccination rates in every country in the world and in the case that we don’t reach herd immunity, it emphasizes the point of vaccination to protect oneself from the high likelihood of exposure to SARS-CoV-2.
How Infectious Can We Be?
The impact of having COVID and infecting others can be easily illustrated with the reproduction number or R0 (R naught). The figure below gives an example if the reproduction number was 4 in which one person will go on to infect 4 people and those 4 people would go on to infect 4 people each.
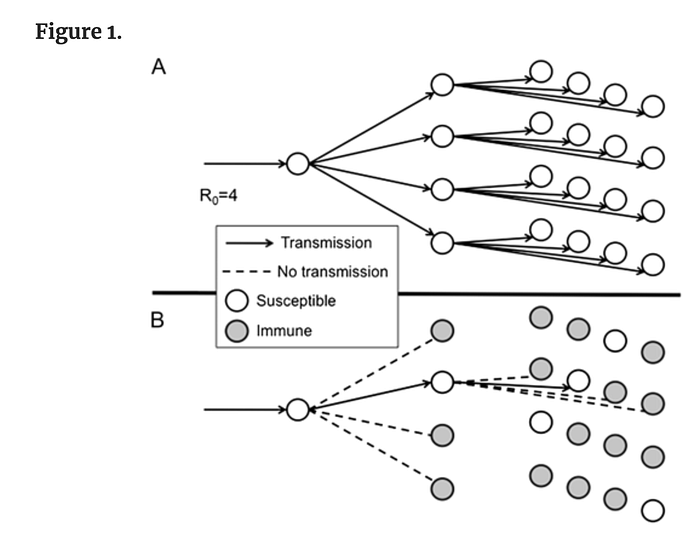
With the current reproduction number for the Delta variant being somewhere between 6 and 8, we can create our estimate for how many people we can potentially infect if we ourselves have COVID. Let’s use the reproduction number of 8 and let’s iterate through 5 rounds as an exercise where 1 person would infect 8 and those 8 would infect another 8 which is the following calculation 8*8*8*8*8=32,768 people. 1 infected, becomes 8 infected, becomes 64 infected, then 512, then 4096, then 32,768. Out of those 32,768, we can expect an estimated 25% would experience long covid which is 8,192 and an estimated 2% will die which is 655. This is just an example of the impact of the Delta variant and it assumes not being vaccinated and not using nonpharmaceutical interventions (NPIs) like masking, social distancing, and ventilation. Using NPIs and being fully vaccinated prevents or reduces these numbers by impacting the level of transmissibility, the likelihood and degree of long covid, and the chances of death.
Viral Load of Breathing, Talking, Singing
A recent study provides further insight into the difference in aerosols produced when it comes to breathing, talking, and singing. They found that earlier in the disease people were more likely to produce detectable virus and that the proportion of virus varied significantly.
The largest proportion of SARS-CoV-2 RNA copies was emitted by singing (53%), followed by talking (41%) and breathing (6%)… overall, fine aerosols constituted 85% of the viral load detected in our study.
This study supports previous studies that show aerosols as the main form of transmission and further highlights the need for nonpharmaceutical interventions like masks, ventilation, and air filtration.
Vaccination Rates and Hospital Capacity
There is clear data that shows low vaccination rates can overwhelm hospital capacity and, in fact, this is already happening in many counties in Missouri, Florida, and Arkansas.
Missouri hospital systems continue to reach capacity. In addition to Green County’s Cox Health, which was the first to send patients to neighboring hospital systems, Mercy Hospital in Springfield had to source additional ventilators from its network and has since added a 6th COVID unit when they only needed 5 units during the last surge. Both Cox Health and Mercy hospitals have requested additional resources from the state which include an alternative care site, staffing for additional beds, and increased capacity for antibody treatment.
On July 17th, the chancellor of the University of Arkansas for Medical Sciences, Dr. Cam Patterson announced that UAMS is at full capacity with COVID-19 patients.
“The hospital is full. COVID-19 numbers increase every day. We are staffing inpatients in the ER and recovery room. No space for transfers. Running out of caregivers. Support health care workers. Mask up. Get vaxxed.”
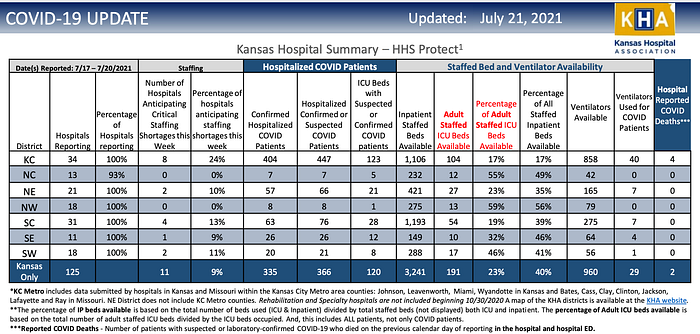
The University of Kansas Health System has also reached capacity. Steve Stites, the Chief Medical Officer shared with the Kansas City Star,
“I think we’re at a tipping point,” the system’s chief medical officer, Steve Stites, said Wednesday, according to The Kansas City Star. “If we don’t take it seriously, we could easily end up back where we were in November…We are turning down transfers, which is creating, I think, a real concern, maybe even a crisis here in our region because patients are having trouble landing into beds anywhere near their hometown,”
Delta = Accelerated Hospital Admissions
Delta’s increased level of transmissibility, its increased ability to evade immunity, and its increased severity accelerate the number of cases and with it the potential amount of people that will be hospitalized. The result of this is we are seeing and will continue to see hospitals reach capacity sooner than during previous waves. The Chief Administrative Officer of Mercy Hospital highlighted this in a recent interview.
“…June 1st we had 26 patients in house, we hit 128 yesterday and 133 today, so in 39 days we made that acceleration. Last year it took us from September 1st to our peak on December 28 to go from 24 to 113, so 150 days. We eclipsed that this year in 39 days.”
To put this into perspective, they are admitting patients around four times as quickly during this wave than in the previous wave. This level of growth is consistent with the original calculation of the Delta variant being nearly four times as transmissible as the original wild-type. It is likely we will continue to see this level of growth across many more counties in the United States with similar vaccination rates. We can expect this growth rate of hospital admissions to slow with higher vaccination rates but the exact rate of change depending on the level of vaccination rates is to be determined and this is further complicated with larger populations who may have higher rates of vaccinations but a large number of people unvaccinated due to their population size.
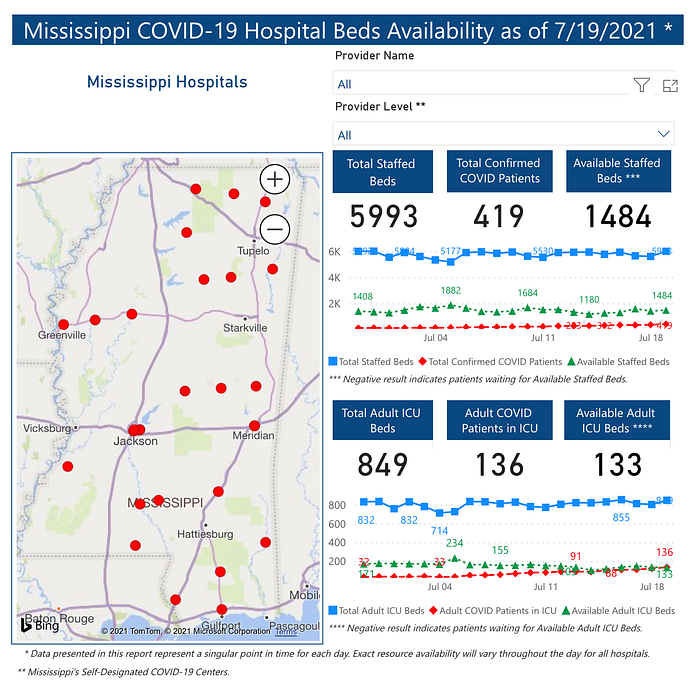
As of July 20, Mississippi currently has 13 ICUs at no capacity and this number is climbing. State Health Officer Thomas Dobbs emphasized the challenges of their situation by saying,
“If you talk to your hospital administrators, docs, ICU docs and ER docs, they’ll tell you we’re getting to a point where we’re actually having to fly patients from the Delta to the Pine Belt to get access to care because there’s really not that much access to it right now.”
This summer, it has taken Mississippi from June 21 to July 18 to go from 103 to 392 daily cases whereas in the previous summer surge it took them from April 1st to June 23rd to get from 100 to 392 daily cases, in other words, 27 days this time compared to 83 days last summer. This means they are currently growing 3 times as quickly as before and this is being reflected in their hospitalizations.
Mississippi’s COVID dashboard highlights the diminishing availability of ICU beds across the state
Will High Vaccination Rates Prevent Hospitals from Becoming Overwhelmed?
What we are seeing is that every state is increasing in cases and hospitalizations at different rates. The reasons for this include prevalence of Delta, vaccination rates, previous immunity from infection, the level of social mixing and social mobility, and the extent to which nonpharmaceutical interventions are being used. Making this projection is complicated because of these variables but a simple attempt would be to take the overall numbers of ICU beds, the number of those currently occupied, and the weekly growth rate of occupied beds.
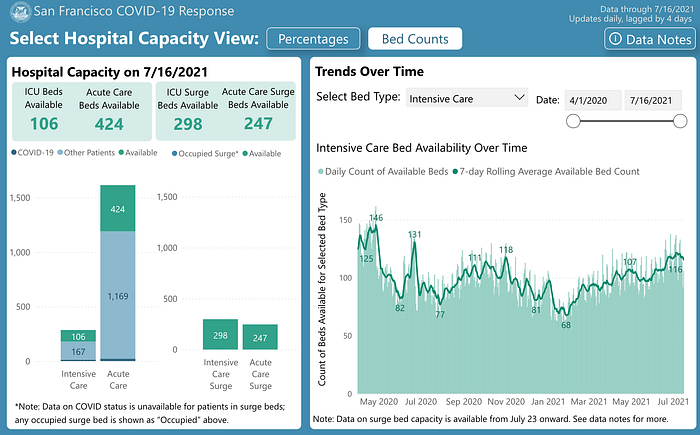
As of July 16, San Francisco County has a total of 273 beds, 167 that were used and 106 that were free. The growth rate from the previous week was 14%. If we calculate for the following week using this growth rate, the total amount of beds used for the following weeks would be 190, 216, 246, and 280, respectively. According to this calculation, we can estimate that ICU capacity would be reached in a week. This calculation doesn’t account for beds being freed up, non-COVID patients needing ICU beds, and the growth rate adjusted per week for improved accuracy, but it gives us an estimate if ICU admissions continue at the recent growth rate.
There are more involved but still imperfect ways to estimate the level of risk for hospitals reaching ICU capacity by including the variables of unvaccinated individuals, the ratio between cases and hospitalizations and ICU admissions in that area, and the potential of ICU admissions based on those numbers.
Even in places with high levels of vaccination rates the risk of reaching ICU capacity exists and should be considered in overall COVID response in order to evaluate and address this risk appropriately.

More Hot Spots, More Problems
As the number of hotspots grows, the issues of resource allocation and the impact on the overall community compound. These resources include healthcare workers, ventilators, beds, and ICU units. Additionally, the services provided for non-COVID patients become strained and can be paused as we saw with elective surgeries during previous surges. Mississippi’s Health Officer Thomas Dobbs highlights this point during his July 20th press briefing,
“It’s not just if you have COVID if you can’t get an ICU,” Dobbs said, It’s if you have a heart attack, or if you have a stroke or if you’re pregnant and you need some emergency care. It’s going to affect everyone. We have once again threatened the healthcare system with the explosion of COVID.”
During previous waves, we also saw a drop in admissions of strokes, heart attacks, and other medical emergencies which many health experts suspected were a result of trying to avoid hospitals in fear of getting COVID. When there are many hotspots across the United States and resources are limited, decisions are made that reduce or prevent adequate care to individuals and people delay receiving important and urgent health services.
Growing hot spots also challenge an already strained healthcare workforce that has experienced 3,600 deaths in the first 12 months of the pandemic and 1 in 10 experiencing long covid. The stress, trauma, and demand of going through this pandemic are highlighted in a recent study that showed 1 in 5 healthcare workers have “moderately or very seriously considered leaving the workforce and about 30% have considered reducing their hours.” Cox Health in Greene County, Missouri highlighted many of these challenges as they recently reached capacity and struggled to recruit traveling nurses and respiratory therapists due to a limited number of those individuals now being unavailable. The author of the study, Angela Fagerlin, reflects in a press release,
“It’s sobering to learn that, during a time of economic recession, at least one-fifth of our workforce were considering leaving their jobs because of the severe levels of stress they were experiencing… people who have spent five to ten years of their adult lives training to do this kind of work. Yet, it’s so overwhelming and burdensome that they were potentially thinking about giving it all up.”
Vaccines Continue to Work
Vaccines continue to show their effectiveness at preventing and reducing symptomatic and severe disease as the overwhelming amount of hospitalizations and deaths are among those unvaccinated. The Associated Press provided an analysis of available government data from May showing that “breakthrough” infections in fully vaccinated people accounted for 1.1% of COVID-19 hospitalizations, fewer than 1,200 of more than 107,000 at the time.
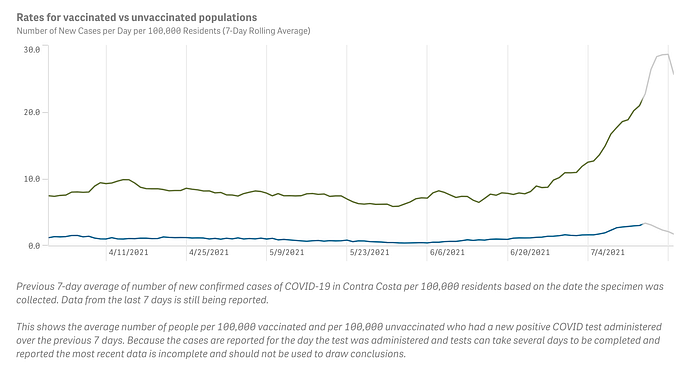
Across the United States, we are seeing the divergence between cases among the vaccinated and the unvaccinated like in Contra Costa County.
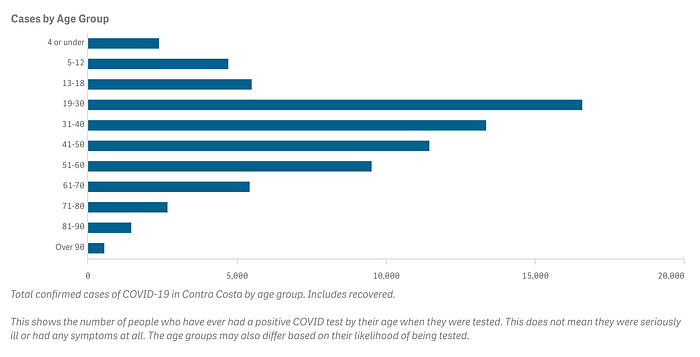
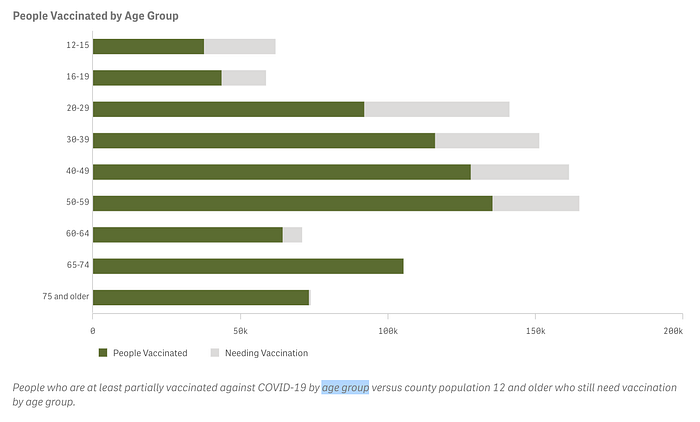
We continue to see cases largely among the younger demographics who have a higher percentage of unvaccinated compared to older demographics.
The Florida Department of Health reported recently that between July 16 and 18, all 1,951 COVID cases over those three days were among the unvaccinated.
In Los Angeles County, recent data shows the overwhelming amount of recent cases and hospitalizations happening amongst those who are unvaccinated.


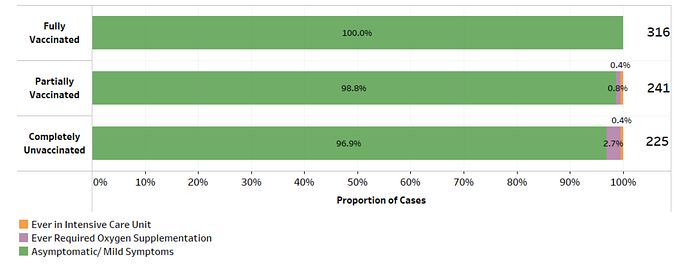
Data from Singapore’s Ministry of Health recent data supports the disproportionate severity and hospitalization among the unvaccinated compared to the vaccinated.

A breakdown of Singapore’s cases based on vaccination status highlights that vaccination helps to prevent serious disease. Over the last 28 days, among the 10 local cases that either required oxygen, were admitted to an ICU, or died, 7 were unvaccinated, 3 were partially vaccinated, and none were fully vaccinated.
COVID Impacts on the Brain
We continue to find the long-term impacts of COVID on the body. A recent study based in the UK showed the impact it can have on the brain by comparing before and after images of the brain through MRI scans that show a loss of grey matter in areas connected to taste and smell.
“Our findings thus consistently relate to loss of grey matter in limbic cortical areas directly linked to the primary olfactory and gustatory system.”
40,000 individuals had been scanned by the UK Biobank before the start of the COVID-19 pandemic which made it possible to invite hundreds of them back to capture a second image of those who had contracted COVID.
Children and COVID
Understanding children’s experience with COVID is a largely neglected area because of observations that they experience less severe disease compared to older individuals. However, understanding children’s experience with covid is important because there is data showing that children experience persisting symptoms known as long covid, hospitalization, and greater rates of death compared to other infectious diseases.
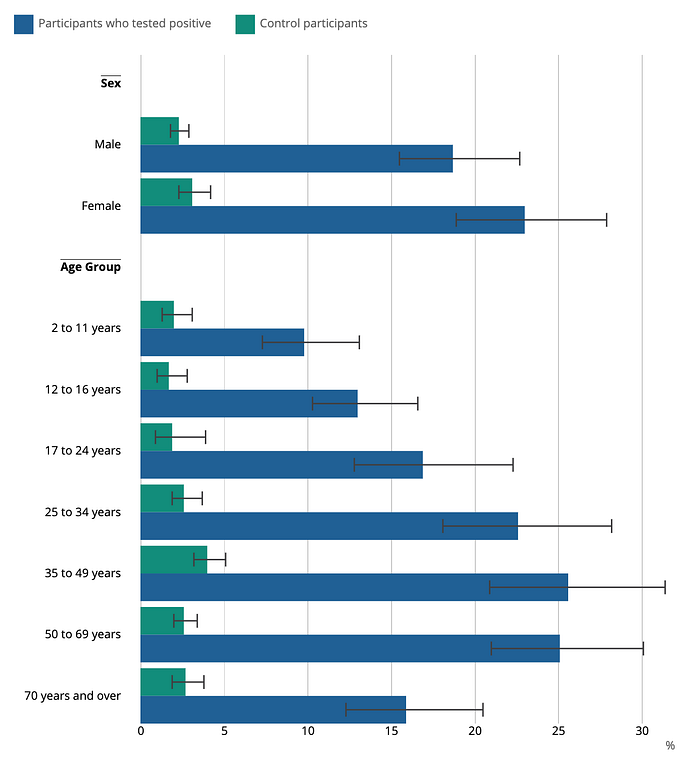
A recent study showed that 4% of children had at least 1 symptom beyond 12 weeks and with the most frequent symptoms being 3% tiredness, 2% difficulty concentrating, and 2% increased need for sleep. Another survey of children with long covid showed that the median time for persisting symptoms was 8.2 months with only 10.0% of children having returned to previous levels of physical activity. The UK Office for National Statistics’s report from April shows that 10–13% of kids have persisting symptoms for 5 weeks or more.
Studies and data are limited and more research is need to understand long covid among children and its health impacts.
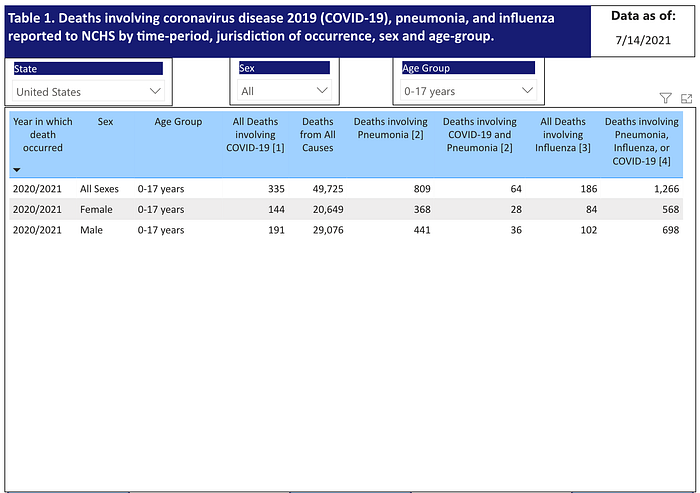
Deaths for children are commonly compared with death rates of older populations but it is helpful to compare it to other infectious diseases within its own age group. When we compare children deaths involving COVID with deaths involving influenza, data from the CDC shows us that about 80% more children deaths involved COVID at 335 compared to 186, respectively.
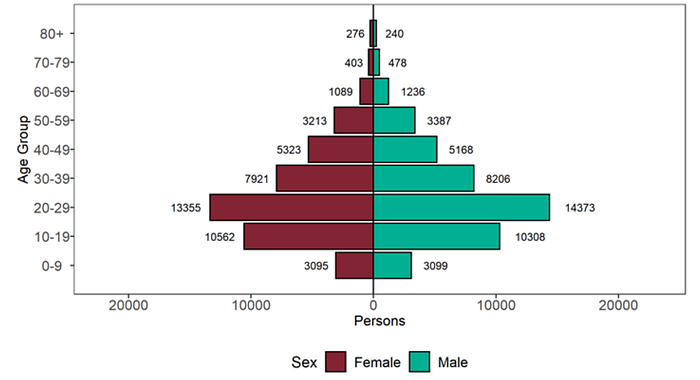
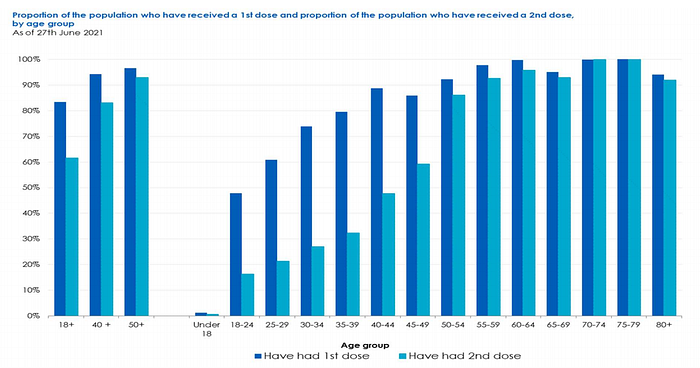
Data from the UK Technical Briefing shows that most cases are amongst the younger demographics largely due to lower vaccination rates and no vaccinations for children 12 and under which suggests that this group remains highly vulnerable during this time.
In addition to the direct health impacts of COVID on children, a recent global study published in the Lancet highlighted the impact of losing parents and caregivers. Between March 1, 2020 and April 30, 2021, the study estimates that 1,134,000 children had experienced the death of at least one parent or custodial grandparent and 1,562,000 children had experienced the death of at least one primary or secondary caregiver. The study goes on to emphasize the emotional and financial impact for these children,
“Orphanhood and caregiver deaths are a hidden pandemic resulting from COVID-19-associated deaths. Accelerating equitable vaccine delivery is key to prevention. Psychosocial and economic support can help families to nurture children bereft of caregivers and help to ensure that institutionalisation is avoided.”
Vaccine Equity: A Humanitarian and Variant Crises
Making sure everyone in the world has access to vaccines is of great urgency to save lives and reduce the likelihood of new variants of concern. With many countries lacking vaccines, the evidence is overwhelming on the spread, hospitalization, and deaths that occur in populations with the presence of the Delta variant.

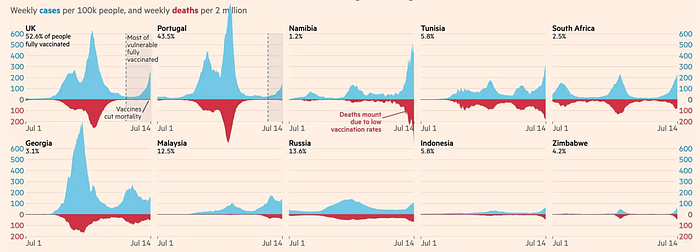
We see in the chart from the Financial Times that the proportion of cases to deaths is significantly higher in unvaccinated countries.
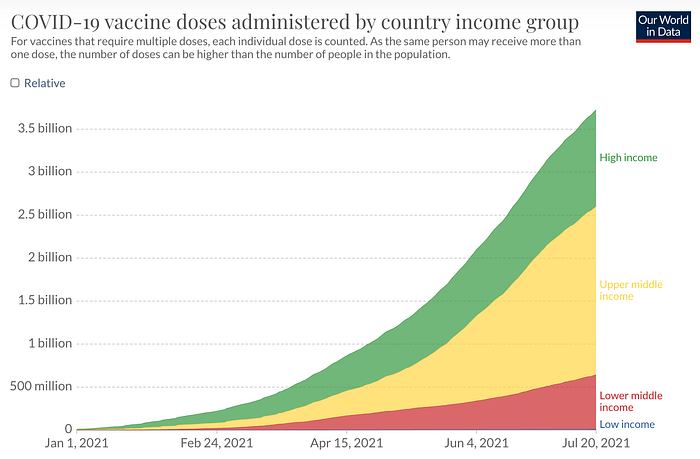
The distribution by country income group shows that high income and upper middle income countries have about 6 times as many doses administered compared the lower middle income and low income countries.
The continent of Africa alone has nearly 1.4 Billion people and less than five countries have more than 10% of their countries with at least one dose.
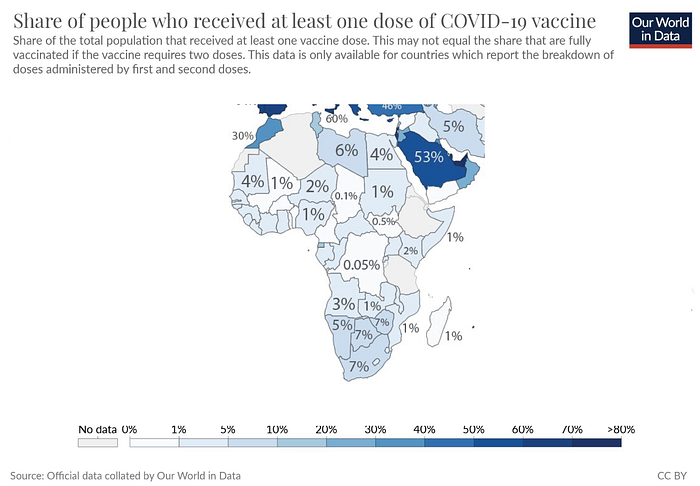
“26.6% of the world population has received at least one dose of a COVID-19 vaccine, and 13.2% is fully vaccinated” — Our World in Data
13.2% of the world fully vaccinated means that roughly 7 billion people remain with little to no vaccine protection and 26.6% of the world only having one dose means that 6 billion people have no vaccine protection. For the world this is a humanitarian crisis, for the countries with higher vaccination rates, this is a risk of variants that can set back the immune protection achieved through vaccination progress.
More Transmission, More Variants
Variants are a natural part of mutations as virus replication occurs. Some of these mutations are inconsequential and fail to gain prevalence while others produce mutations that become a variant of concern because of increased transmissibility, increase severity, or increased immune escape. In the case of Delta, early data shows an increase in all three of these areas with severity showing increased hospitalization while we wait to understand if this also includes increased death. Transmission has produced mutations which have produced other variants of concern like Alpha, Beta, and Gamma. With transmission continuing to be high and an overwhelming amount of the global population continuing to be unvaccinated, this environment is set to create immense levels of replication and mutations, increasing our chances of seeing more variants of concern.
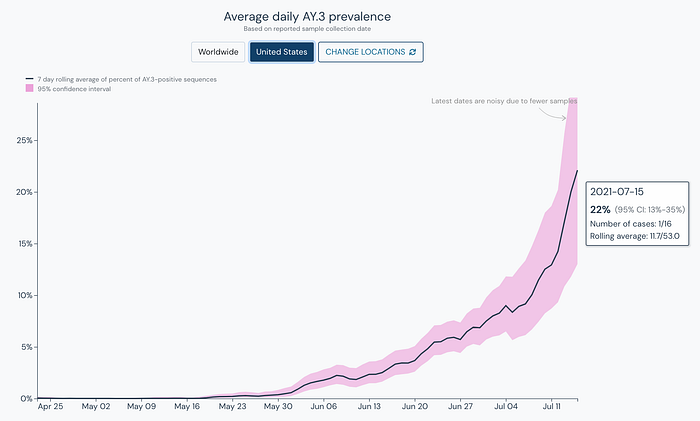
Introduction: Delta sublineage AY.3
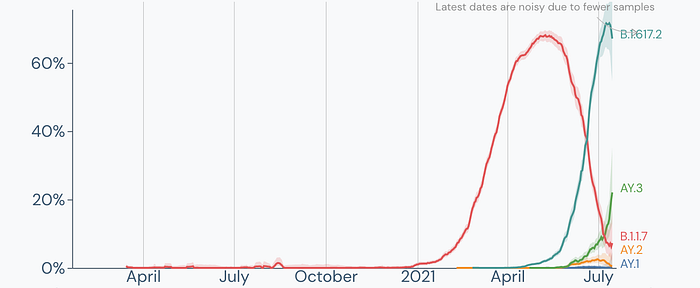
Delta (B.1.617.2) currently has three sublineages, AY.1 (Delta Plus), AY.2, and now AY.3 which currently has an estimated prevalence of 22% in the United States based on the latest genomic sequencing data.
While it appears that Delta Plus (AY.1) and AY.2 have been currently outcompeted by Delta, AY.3 is continuing to rise in prevalence while other variants have continued to decrease. Data from Mississippi shows AY.3 has been outcompeting Delta.
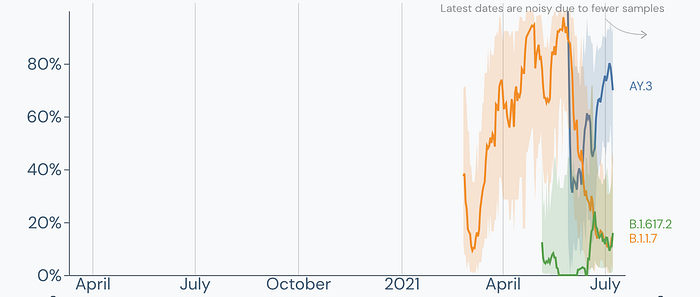
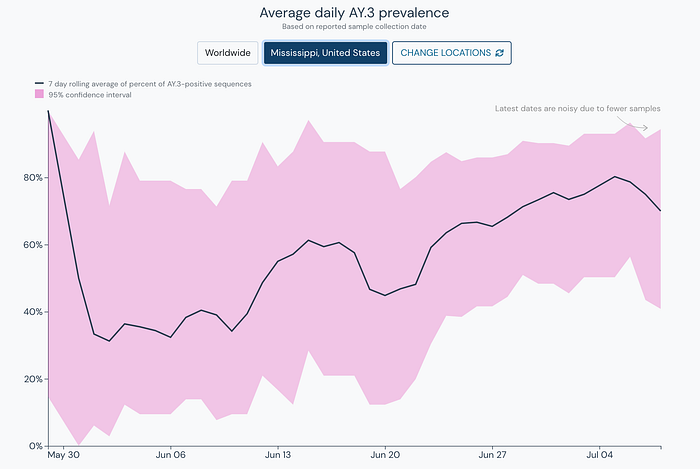
AY.3 has clearly become the dominant strain in Mississippi outpacing both Alpha (B.1.1.7) and Delta (B.1.617.2).
When we look at the overall chart for the United States we also see AY.3 continuing to growing in prevalence.
It is too early to say definitively that it will become the dominant variant of the Delta sublineages especially due to conflicting data with AY.3 in neighboring states, high levels of prevalence in Missouri but lower levels in Arkansas. It is worth noting that this region has been the epicenter for the recent surge partly due to low vaccination rates and to be determined if AY.3 played a part as well. AY.3 is worth observing and we will have a clearer picture of this Delta sublineage in the coming weeks.


Mask and Vax
With the World Health Organizations’s recommendation for everyone regardless of vaccination status to mask and several counties in California following their lead, there is still not national adoption of this recommendation across states nor from the CDC.
A recent Gallup poll showed that since March, masking has dropped 19% by those fully vaccinated and has dropped a significant 35% by adults who are not vaccinated.
“Longer term, mask-wearing has fallen more sharply among nonvaccinated adults (down 34 points since March) than among those who are fully vaccinated (down 19 points).” -Gallup
In some states, like Arizona and Georgia, the governors have signed laws to restrict schools from mandating masks. Recent outbreaks in summer camps show a preview of what we can expect. A recent report by ABC highlighted outbreaks occurring in Texas, Illinois, Florida, Missouri, and Kansas.
“In the Houston area, health officials reported more than 130 youths and adults tested positive for the virus in cases connected to a church camp. The pastor of Clear Creek Community Church in League City said the outbreak happened in two waves, first at the camp and then when people returned home in late June… In Illinois, health officials said 85 teens and adults at a Christian youth camp in mid-June tested positive, including an unvaccinated young adult who was hospitalized, and some people from the camp attended a nearby conference, leading to 11 additional cases.”
An epidemiologist at the University of Arizona, Dr. Elizabeth Jacobs, highlights the issues with the ban on mask mandates in Arizona schools,
“It is critical that we maintain masking indoors for all individuals, whether vaccinated and unvaccinated, in areas with high SARS-CoV-2 transmission. This includes many parts of Arizona, where schools have already begun with the majority of students unmasked. The ban on mask mandates in schools implemented by Governor Ducey will likely result in unsustainable pupil and staff absences, in addition to more morbidity and mortality in a state that has already been through two devastating waves.”
The American Academy of Pediatrics recently updated their guidelines on masking aligned with the World Health Organization by stating in a press release,
“In addition to vaccinations, the AAP recommends a layered approach to make school safe for all students, teachers and staff… That includes a recommendation that everyone older than age 2 wear masks, regardless of vaccination status.”
Maria Van Kerkhove, the World Health Organization’s Technical Lead on COVID-19 addresses the lack of masking as part of the challenges they’ve identified as “inappropriate use of public health and social measures.”
When you take into context the 147 million who remain unvaccinated, children under 12 who cannot get vaccinated, the immunocompromised and immunosuppressed who do not mount a sufficient immune response to be protected with the vaccine, the reduction in the vaccine’s effectiveness against infection by Delta, the ability for someone infected by Delta to produce around 1000 times more viral load than the original wild-type that started the pandemic, the ability for the Delta to infect more easily, and the social impact of dropping indoor masking policies that resulted in over a 1/3 of those unvaccinated dropping their masking practices, the recommendation by the World Health Organization will help to reduce transmission as cases and hospitalizations are surging throughout the country.
What’s next?
What we do now will greatly determine the outcomes of the next months. With our drastically reduced vaccination rates and the time it takes to build immunity after receiving the needed doses to become fully vaccinated, implementing nonpharmaceutical interventions nationally like indoor quality masking is urgently needed to have the quickest impact possible to suppress transmission of the Delta variant and any of its potentially problematic sublineages. At our current growth rate and with 147 million not fully vaccinated, not acting quickly enough will result in the possibility of having us reach the peak of our winter surge within the next 30 days, an outcome that will prevent COVID patients from getting adequate care and strain the healthcare system putting many who need medical treatments or have emergencies at risk. As schools open up, a national mask mandate would protect many who would be vulnerable in those environments and provide support for schools where some governors are restricting mask mandates in schools. There are many who remain vulnerable to long-term disease and death in the U.S and around the world, and record levels of transmission will expose them to Delta and in the process put us at risk of new variants, potentially like Delta’s sublineage AY.3 or others that emerge, that reduce the effectiveness of our vaccines through enhanced immune escape, transmissibility, and or severity.
We have an opportunity to change things around quickly and we can do this by using every tool available to us and most immediately tools that quickly suppress spread like implementing quality mask recommendations for indoor use like N95s, increasing ventilation and air filtration, and investing in access and trust to increase vaccination in more communities. Additional tools to control the pandemic include increasing genomic testing to learn about new variants quicker, testing everyone regardless of vaccination status after exposure to improve data on vaccine effectiveness against new variants and increase data on secondary infections, robust contact tracing, and isolation protocols for the sick. We have every tool we need to save lives now, we need to urgently act and use them.
